
Trauma to the growth plate (red arrow) in the wrist of a gymnast from repetitive force.
Description
The growth plate in bones is called the physis. Almost every bone has a physis. The physis is made of specialized cartilage and is located near the ends of the long bones. Because cartilage is not calcified, it looks like a dark line in the bone on the X-ray. The physis helps the bone grow, both in length and width. When a child stops growing, the physis hardens into solid bone. Boys generally stop growing around 16 years of age, and girls around 14 years of age, although this varies greatly.
Fractures in the physis often occur because the cartilage is weaker than the hard bone. In fact, the physis is weaker than the ligaments that connect the 2 bones in a joint. Because the physis is very active (since it helps the bone grow!), fractures through the physis heal very quickly. It is important to bring your child to see an orthopaedic doctor within the first 5 to 7 days of injury if there is a fracture through the physis. If the bone needs to be manipulated, there may be so much healing in a physeal fracture by 10 days that the bone cannot be moved.
Physeal fractures are common; they make up 15-30% of all fractures in children. Common areas for fractures are the fingers, wrist, and lower leg. These often occur from an acute trauma, but stress fractures through the growth plate can be seen with chronic overuse, such as in gymnasts and pitchers.
Because of the risk of problems in growth, it is important to bring your child to see an orthopaedic doctor if there is physeal fracture.
Types of Physeal Fractures
The Salter-Harris classification is used to describe the pattern of physeal fracture.
Type I fractures – these occur through physis. The fracture may be just a crack in the physis that is still in perfect alignment, or the physis may be completely disrupted and the bone separated.
Type II fractures – these fractures go partly through the physis and then out the shaft of the bone away from the joint.
Type III fractures – these fractures go partly through the physis and then exit the end of the bone into the joint. The joint surface may be disrupted.
Type IV fractures – These fractures go through the shaft of the bone, through the physis, then exit out the end of the bone at the joint.
Type V fractures – These are crushing injuries through the physis and can be very difficult to see on X-ray.
Symptoms
A crooked limb, swelling, pain, an inability to move the limb, and bruising are the most obvious signs that there is a fracture. Pain that does not get better on its own may also be a sign of a fracture, even if the arm does not look crooked.
Examination
The doctor will carefully look at the areas around the injury as well as touch those areas to see what hurts. He or she may also try to gently move the joints. Testing the nerves and circulation are also important.
Other Tests
Most of the time, simple x-rays and an examination are all that are needed to diagnose a physeal fracture. Occasionally, the doctor may need to order a MRI or CT scan.
Treatment
Treatment depends on which bone is broken, the age of your child, and the pattern of the injury. May of these fractures can be treated in a cast, but some require surgery and metal pins or screws to hold the alignment. If the fracture involves the joint, surgery is often needed to make sure the joint surface and physis are lined up.
Physeal stress fractures heal with rest, although often a splint or cast may be used to help the pain. After healing, your child should try decrease amount of time spent on the activity that caused the stress fracture, to prevent the stress fracture from happening again. For example, a pitcher should limit pitch counts, and a gymnast should decrease time at the gym.
Surgical Treatment
Surgery may be needed in some circumstances:
- There is a cut in the skin near the broken bone
- The fracture is too far out of place or will not stay lined up even in a cast
- The bones have started to heal in a bad position and cannot be manipulated because of the healing.
Different types of implants may be used in surgery to keep the bones aligned. This may include temporary pins or plates and screws. After surgery, a cast or splint may still be used to help keep the bones in place during healing.

13 year old child with Salter-Harris II distal tibia and fibula ankle fractures.

Healing after a screw was placed to line the bones back up.
Outcome
Growth plate fractures, especially in the femur (the upper part of the knee), must be followed for at least 9 to 12 months after the injury to make sure the bone continues to grow properly. Repeat X-rays are needed to look for this.
If a bony bridge forms across the physis, the growth plate will stop growing or may start growing crookedly. Luckily, this is rare. In those cases, your doctor may recommend surgery to try to prevent or correct deformity. The treatment can vary depending on how much of the physis has stopped growing and how old your child is. Different techniques include removing the bony bridge and inserting fat into the that area, cutting the bone and re-aligning it, or completely stopping the growth in the rest of the physis as well as the physis in the other leg so that one leg does not grow longer than the other. In very rare cases, surgery may consist of lengthening the bone.
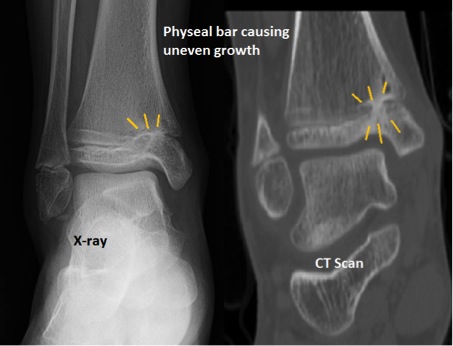
6 months after an ankle fracture in the growth plate, one part of the growth plate has stopped growing. The ankle is starting to grow crookedly.
More Information
Page QR Code:





