Overview
Children are active, and this can lead to a child falling onto their arm, leading to a fracture. If your child falls fast enough and with enough pressure, the bone around the elbow may break. Elbow fractures in children are very common and make up about 10% of fractures in kids.
Anatomy
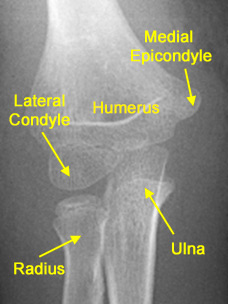
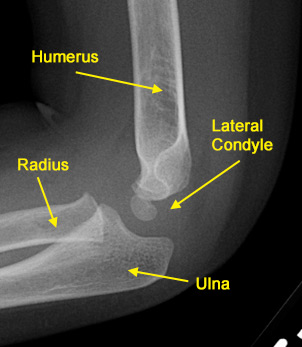
There are 3 bones in the elbow joint. The relationships between the bones are important because they allow the elbow to not only bend and straighten, but also allow the forearm rotate (palms up and palms down).
- The humerus is the bone in the upper arm and goes from the shoulder to the elbow.
- The radius is the forearm bone that goes from the elbow to the wrist and is on the thumb side of the forearm. This is the bone that rotates when you rotate your wrist palms up and palms down.
- The ulna is the other forearm bone from the elbow to the wrist and is on the pinky side of the forearm. This bone is the hinge in the elbow that allows bending and straightening.
Types of common elbow fractures
Occult elbow fractures are very common in growing children. A fall may result in quite a lot of swelling and pain in the elbow region and yet the first x-rays often don’t show an obvious fracture. Swelling in the elbow region may be visible as a ‘fat pad sign’ on the x-ray indicating bleeding in the elbow joint. Up to 75% of these children will go on to have visible healing bone on later x-rays (2-3 weeks later) and often these injuries are protected in splints or casts. Rapid healing and much improved comfort is expected when the injury is protected in a cast or splint.
Depending on how your child falls, there can be several places that can be injured in the elbow.
Supracondylar fracture:
This occurs in the humerus, just above the elbow. This is the most common elbow fracture, but may need urgent surgery if the fracture is very severe.
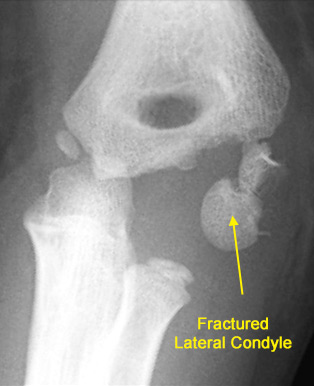
 Condylar fracture:
Condylar fracture:
This fracture occurs in the humerus, just above the elbow, but involves the joint surface. Usually, this fracture occurs on the outer part of the elbow where there is a bony prominence. This is known as a lateral condyle fracture. Lining up the joint surface is an important part of treating these fractures. Lateral condyle fractures often require a slightly longer amount of time in a cast than other elbow fractures and must be followed closely because sometimes they do not heal.
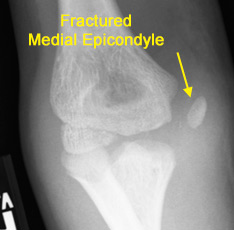
 Epicondylar:
Epicondylar:
This fracture occurs at either tip of the bony prominences on the inside inner (medial) and outside outer (lateral) of the elbow. Medial epicondyle fractures may occur with elbow dislocations but can also happen with overuse that stresses the bone, such as with baseball pitchers.
 Physeal fractures:
Physeal fractures:
These fractures occur through the growth plate. In the elbow, this can occur in the humerus, radius, or ulna, and can lead to problems in the bone growing properly if the fracture is not treated correctly. See also
physeal fractures.
Monteggia fractures:
This occurs when the ulna has a fracture and the radial head (the part of the radius near the elbow) has dislocated from the elbow joint. Children can have this injury without an obvious fracture but will have significant pain, swelling, and difficulty moving the elbow. A pediatric orthopedic surgeon (LINK) can diagnose this injury on an exam and evaluation of the x-rays. Rarely would any other test be necessary such as MRI or CT scan.
Symptoms
Crookedness, swelling, acute pain, an inability to move the elbow, and bruising are the most obvious signs that there is a fracture. You should bring your child to see a doctor if this happens. Severe injuries may also be accompanied by numbness and tingling in the hand or forearm. In this case, you should bring your child to the emergency room immediately. Pain that does not get better on its own may also be a sign of a fracture.
Figures – These children have severe supracondylar humerus fractures with bruising, swelling, and deformity. These patients should be brought to the emergency room immediately.



Examination
The doctor will carefully look at the skin around the elbow, forearm, and wrist as well as touch those areas to see what hurts. He or she may also try to gently move the joints. Testing the nerves and circulation to the hand are also important.
Other Tests
Most of the time, simple x-rays are all that are needed to diagnose an elbow fracture. Because forearm fractures can be associated with elbow fractures, your doctor may obtain x-rays of those areas as well.
In very young children, the bones in the elbow are still soft and made of cartilage and do not show up on the x-ray yet. When that happens, your doctor may also order x-rays of the other elbow for comparison. In rare cases, an MRI, ultrasound, or an arthrogram, where dye is injected into the joint, may be needed to see the bones and the joint surfaces.
Treatment
Depending on the type of fracture and how big the gap is between the broken bones, treatment may be as simple as a sling or may require urgent surgery. The elbow region has much less growth potential and can not grow and correct angulation or displacement unlike at the wrist or shoulder region in young children. It is much harder to come back later after the fracture has healed and correct the bone alignment compared to having the fractures heal in proper alignment with surgery.
Nonsurgical treatment:
If the bones are lined up relatively well, your doctor may recommend treatment in a cast or splint for about a month. A repeat x-ray at a week after injury is sometimes needed to make sure the bones do not shift out of place.
Surgical treatment:
If the bones do not line up, your doctor may recommend setting the bones to get them back in place. Occasionally, this can be done without surgery. More often, pins, screws, or wires are required to hold the bones lined up for about a month while they heal. A cast or splint is often used for extra protection after surgery. Usually the pins are temporary and will be taken out after the bone is healed. Depending on the type of fracture, there is often enough healing in a month to allow your child to start moving their elbow without a cast.
Outcome
Stiffness in the elbow and/or wrist is common after coming out of the cast or splint, especially after surgery. This usually gets better on its own after a few months, but sometimes physical therapy is needed to help regain motion. If the bones are lined up well, the long-term outcome is generally excellent, even if there is still a mild loss of motion. If the bone does not heal or heals in the wrong position, the elbow will look crooked and have loss of motion. This can be avoiding by bringing your child to see a doctor promptly if you think they have an elbow fracture.
More Information
Page QR Code:


